
- Подход RCA
- Введение
- Описание
- Цель
- Процесс анализа первопричин
- Идентификация причин
- Важность
- Услуги анализа RCA
- Процесс внедрения RCA
- Результаты
- Поддержка
- ПО для RCA
- Заключение
- Сбор, организация и анализ информации
- Анализ защитных механизмов
- Transition to corrective actions
- Manufacturing and industrial process control
- IT and telecommunications
- Health and safety
- Abstract
- Background
- Method
- Results
- Conclusion
- Introduction
- Root cause analysis
- The Norwegian regulatory regime for qualitative improvement and RCA
- Methodology
- Design
- Setting and sample
- Data collection
- The process of thematic coding
- Ethical approval
- Results
- Case description (The RCA team’s summary from the final report)
- Theme: The management system
- Quality management department’s role in the RCA process
- Scattered documentation
- Theme: External and internal assessment
- Composition of the RCA team
- Police work interrupting the RCA process
- Using colleagues to provide external medical expertise is seen as challenging for the process and the participants
- Theme: Being an RCA team member
- Role challenges
- Ambivalence about being an RCA team member
- Discussion
- Implications for practice
- Study strengths and limitations
- Future research and development
- Conclusion
- Availability of data and materials
- References
- Acknowledgements
- Funding
- Author information
- Authors and Affiliations
- Contributions
- Corresponding author
- Ethics declarations
- Ethics approval and consent to participate
- Consent for publication
- Competing interests
- Additional information
- Publisher’s Note
- Rights and permissions
- About this article
- Cite this article
- Keywords
Подход RCA
Введение
Анализ первопричин (Root Cause Analysis, RCA) – это процесс проведения систематического анализа для выявления фундаментальных или глубинных причин инцидента, сбоя или проблемы.
Описание
Коренная причина — это основная проблема, которая приводит в движение всю причинно-следственную реакцию, в конечном итоге приводящую к проблеме (проблемам).
Цель
Анализ первопричин проблемы — это эфективный способ адекватного устранения проблемы, а не просто лечения ее симптомов.
Процесс анализа первопричин
Процесс анализа первопричин отказов состоит из последовательных формализованных шагов:
- Определение проблемы;
- Сбор данных;
- Определение причин проблемы;
- Определение мероприятий для устранения проблемы;
- Подготовка плана мероприятий;
- Контроль выполнения мероприятий;
- Закрытие проблемы.
Идентификация причин
Идентификация факторов, способствующих отказу систем, или причин, его вызывающих, позволит выработать план действий по устранению проблем.
Важность
Развитие культуры постоянного совершенствования поможет избегать повторения отказов в будущем.
Услуги анализа RCA
Эксперты ООО Эр Би Ай Концепт располагают всеми необходимыми компетенциями и инструментами для внедрения системы поиска и устранения первопричин отказов (RCA) в активах заказчиков.
Процесс внедрения RCA
Процесс внедрения RCA состоит из следующих шагов:
- Демонстрация преимуществ использования системы поиска и устранения первопричин отказов (RCA) для технических руководителей компании.
- Подготовка стандартов предприятия (регламент, инструкции) по RCA.
- Обучение сотрудников компании Заказчика.
- Проведение анализа RCA в одном из активов Заказчика составом обученных специалистов Заказчика.
- Участие в подготовке плана внедрения RCA в активах компании Заказчика.
Результаты
Реализация мероприятий позволяет определять степени влияния первопричин на бизнес компании и снижать эксплуатационные затраты.
Поддержка
По желанию заказчика, после внедрения системы RCA, инженеры Эр Би Ай Концепт продолжат осуществлять техническую и экспертную поддержку.
ПО для RCA
В настоящий момент в нашей компании завершается разработка специализированного программного обеспечения по сбору данных и протоколированию процесса анализа первичных отказов (RCA).
Заключение
Применение RCA поможет повысить эффективность и надежность работы оборудования, а также снизить операционные расходы.
От них во многом зависят оперативность поиска корневых причин отказов оборудования и реализация мероприятий по устранению этих причин отказов.
Отличным способом посмотреть на картину проактивных/реактивных действий является рассмотрение модели оценки рисков Бабочка. В центре модели находится событие или авария. Слева находятся предвиденные опасности и линия защиты, созданная для предотвращения того, чтобы эти опасности привели к событиям. Линия защиты – это регулятивные требования, применимые процедуры, физические барьеры и кибер-барьеры, которые существуют для управления операциями и предотвращения событий. Отличным способом использования анализа корневой причины является превентивная оценка эффективности этих защит путем сравнения фактической производительности с применимыми требованиями, идентификации разрывов в производительности, а затем закрытия этих разрывов для укрепления защиты. Если происходит событие, то мы находимся на правой стороне модели, реактивной стороне, где акцент смещается на идентификацию корневых причин и смягчение ущерба.
Сравните это с расследованием, которое не находит корневую причину: замена предохранителя, подшипника или насоса для смазки, вероятно, позволит машине продолжить работу еще некоторое время. Но существует риск того, что проблема просто повторится, пока не будет решена корневая причина.
Стоит учитывать издержки не только финансовые, но и персонал, который управляет оборудованием. В конечном итоге цель – предотвратить простой; но более того, предотвратить катастрофические травмы. Превентивное начинается с принятия мер по проактивной защите.
Пример метода анализа корневой причины:
- Идентификация и описание: Эффективные утверждения о проблемах и описания событий (как, например, отказы) являются полезными и обычно требуются для обеспечения проведения соответствующего анализа корневой причины. Утверждения о проблемах являются Северной Звездой анализа корневой причины, поскольку они удерживают команду на должной траектории и предотвращают отклонения.
Сбор, организация и анализ информации
Большинство анализов причин и обстоятельств начинаются с сессии сбора фактов для собирания доступной информации, такой как показания свидетелей, хронология событий и применимые требования для происходивших событий во время происшествия. Эта информация может использоваться для установления последовательности событий или временной линии событий, а также для определения защитных мер, которые должны были предотвратить событие (такие как административные требования и физические и кибернетические барьеры). Также следует проверить и проанализировать доступные базы данных (такие как базы данных программы корректирующих действий и программы безопасности) и использовать инструменты анализа данных, такие как диаграммы Парето, карты процессов, деревья ошибок и другие инструменты, которые помогут нам понять пробелы в работе. Можно использовать любое количество инструментов анализа данных, включая инструменты анализа данных Lean Six Sigma, статистические инструменты, а также другие инструменты, такие как иерархическая кластеризация и решения по майнингу данных (например, майнинг данных на основе графовой теории). Еще один подход заключается в сравнении ситуации, находящейся под расследованием, с прошлыми ситуациями, хранящимися в библиотеках дел, с использованием инструментов на основе случайного рассуждения, что может включать в себя анализ изменений, сравнительный временной анализ и анализ задач.
Анализ защитных механизмов
После определения защитных мер, которые должны были предотвратить событие или несчастный случай, очень рекомендуется провести анализ защитных мер (традиционно называемый анализ барьеров) в каждом случае, включая не-анализ причин и обстоятельств. Один из методов заключается в составлении списка защитных мер на диаграмме или виртуальной доске. Затем, для каждой защиты, просматриваем информацию и данные, которые были собраны, в поисках доказательств эффективности этого защитного механизма. Мы фактически ищем недостатки или пробелы в работе, когда административные требования не были выполнены, или когда физические или кибернетические барьеры были обойдены. Исходные пробелы в работе являются всего лишь симптомами более глубоких причин. Мы используем эти симптоматические пробелы в работе, чтобы разработать линии вопросов для дальнейшего исследования, преследуя симптомы обратно к их источникам (то есть корневым причинам) с использованием анализа причин и следствий.
Generating focused, unbiased lines of inquiry questions: After gathering available information, organizing it into charts with timelines and other data, after analyzing available data, and after conducting an analysis of our defenses, we use those insights to generate great questions. These questions will become our lines of inquiry for cause-and-effect analysis. The questions must be unbiased, and to prevent any bias from the RCA team from tainting the investigation, questions should be tied to a specific defense, or to a specific insight from our data analysis (e.g., Pareto charts, process maps, fault trees, control charts) and other tools that provide us with insights into performance gaps. There should not be any curiosity questions, questions that reflect "confirmation bias" (i.e. asking a leading question so they answer what the RCA team thinks are the causes), or questions that are accusatory in nature that will cause those helping the investigation to close down and withdraw.
Cause-and-Effect Analysis: Once we have developed a robust set of lines of inquiry questions from the factual evidence collected, the applicable requirements, and an analysis of the available data, we can take those questions to the organization’s subject matter experts. This begins the process of cause-and-effect analysis. Once we pose a question to the affected organization, we use their answer to pose a follow-up Socratic questions. Socratic questions keep the investigation flowing down to the next deeper causal factors until the organization runs out of answers, or the last causal factor is beyond the organization’s control. There are many skills involved in conducting an effective cause-and-effect analysis, including facilitation skills, communication skills, and Socratic questioning. When conducted properly, this will take the RCA down to the deepest-seated root causes. A word of caution: Ishikawa or the Fishbone Diagram, and the 5-Whys methods, are not rigorous enough for conducting a root cause analysis. The Fishbone is from the 1940s and the 5-Whys is from the 1930, and there are much more advanced methods available. Look for methods that were developed in this century (the year 2000 and later), as they are more likely to account for the new dynamics of the modern sociotechnical work environments.
Charting the Results of the RCA: The best way to chart the results of an RCA investigation is to start populating the final chart from the start. This process has become much easier with the advent of virtual white boards. In a single virtual white board, we can display the timelines, the lines of defenses, the data analysis, the lines of inquiry questions, the cause-and-effect analysis, the root causes, and the corrective action plan.
Corrective Actions to Prevent Recurrence: From a management perspective, the RCA effort is not complete without a comprehensive corrective action plan to address the root causes, the contributing factors, and the "Extent of the Causes." The corrective action plan should be developed by the issue owners and does not require participation by the RCA team, although the team is an excellent source of guidance for the issue owners. The Extent of Cause reviews are conducted to determine the extent of the damage or impact that the root causes and contributing factors had on humans, equipment, or facilities. Extent of Cause reviews are an Achilles heel in the vast majority of organizations and a primary reason why RCAs and corrective action plans fail to prevent recurrence. Also, care must be taken to avoid corrective action plans that simply add more administrative requirements and more training to the organization. To avoid this, use the Hierarchy of Hazard Controls and Lean Mistake Proofing as guidelines for developing effective corrective actions that have a much higher likelihood of preventing recurrence.
Effectiveness Reviews: After a pre-determined period after the implementation of the corrective action plan, an effectiveness review is scheduled to evaluate the effectiveness of those corrective actions. This requires specifying a set of metrics or indicators that will be monitored prior to and after the corrective actions are implemented, so we can measure their impact. If the desired results are not achieved, which in most cases is a significant reduction in the magnitude or frequency of the event or problem, then the RCA must be reopened as it was not effective.
Transition to corrective actions
The goal of RCA is to identify the root cause of the problem with the intent to stop the problem from recurring or worsening. The next step is to trigger long-term corrective actions to address the root cause identified during RCA, and make sure that the problem does not resurface. Correcting a problem is not formally part of RCA, however; these are different steps in a problem-solving process known as fault management in IT and telecommunications, repair in engineering, remediation in aviation, environmental remediation in ecology, therapy in medicine, etc.
Root cause analysis is used in many application domains. RCA is specifically called out in the United States Code of Federal Regulations in many of the Titles. For example:
TITLE 10 – ENERGY >>> 10CFR Part 50, Appendix B, Criterion XVI, “Corrective Actions” (also adopted by NQA-1)
“Measures shall be established to assure that conditions adverse to quality such as failures, malfunctions, deficiencies, defective material and equipment, and non-conformances are promptly identified and corrected.
In the case of significant conditions adverse to quality, the measures shall assure that the cause of the condition is determined, and corrective action taken to prevent recurrence.”
TITLE 14 – AERONAUTICS AND SPACE >>> 14 CFR Chapter III, Subchapter C, Part 437, Subpart C, §437.73 Anomaly recording, reporting and implementation of corrective actions.
A permittee must record each anomaly that affects a safety-critical system, subsystem, process, facility, or support equipment.
A permittee must identify all root causes of each anomaly and implement all corrective actions for each anomaly.
TITLE 21 – FOOD AND DRUG >>> 21 CFR Subpart J: 21CFR820.100(a) – Corr./Preventive Action: (A) Each manufacturer shall establish and maintain procedures for implementing corrective and preventive action. The procedures shall include requirements for:
Investigating the cause of nonconformities relating to product, processes, and the quality system;
Identifying the action(s) needed to correct and prevent recurrence of non- conforming product and other quality problems;
Verifying or validating the corrective and preventive action to ensure that such action is effective and does not adversely affect the finished device;
TITLE 42 – PUBLIC HEALTH >>> 42 CFR PART 488, SURVEY, CERTIFICATION, AND ENFORCEMENT PROCEDURES > Subpart E—Survey and Certification of Long-Term Care Facilities
§488.61 Special procedures for approval and re-approval of organ transplant programs.
…Root Cause Analysis for patient deaths and graft failures, including factors the program has identified as likely causal or contributing factors for patient deaths and graft failures;
Manufacturing and industrial process control
The example above illustrates how RCA can be used in manufacturing. RCA is also routinely used in industrial process control, e.g. to control the production of chemicals (quality control).
RCA is also used for failure analysis in engineering and maintenance.
IT and telecommunications
Root cause analysis is frequently used in IT and telecommunications to detect the root causes of serious problems. For example, in the ITIL service management framework, the goal of incident management is to resume a faulty IT service as soon as possible (reactive management), whereas problem management deals with solving recurring problems for good by addressing their root causes (proactive management).
RCA is also used in conjunction with business activity monitoring and complex event processing to analyze faults in business processes.
Its use in the IT industry cannot always be compared to its use in safety critical industries, since in normality the use of RCA in IT industry is not supported by pre-existing fault trees or other design specs. Instead a mixture of debugging, event based detection and monitoring systems (where the services are individually modelled) is normally supporting the analysis. Training and supporting tools like simulation or different in-depth runbooks for all expected scenarios do not exist, instead they are created after the fact based on issues seen as ‘worthy’. As a result the analysis is often limited to those things that have monitoring/observation interfaces and not the actual planned/seen function with focus on verification of inputs and outputs. Hence, the saying "there is no root cause" has become common in the IT industry.
Health and safety
RCA is also used in change management, risk management, and systems analysis.
Without delving in the idiosyncrasies of specific problems, several general conditions can make RCA more difficult than it may appear at first sight.
First, important information is often missing because it is generally not possible, in practice, to monitor everything and store all monitoring data for a long time.
Second, gathering data and evidence, and classifying them along a timeline of events to the final problem, can be nontrivial. In telecommunications, for instance, distributed monitoring systems typically manage between a million and a billion events per day. Finding a few relevant events in such a mass of irrelevant events is asking to find the proverbial needle in a haystack.
Third, there may be more than one root cause for a given problem, and this multiplicity can make the causal graph very difficult to establish.
Fourth, causal graphs often have many levels, and root-cause analysis terminates at a level that is "root" to the eyes of the investigator. Looking again at the example above in industrial process control, a deeper investigation could reveal that the maintenance procedures at the plant included periodic inspection of the lubrication subsystem every two years, while the current lubrication subsystem vendor’s product specified a 6-month period. Switching vendors may have been due to management’s desire to save money, and a failure to consult with engineering staff on the implication of the change on maintenance procedures. Thus, while the "root cause" shown above may have prevented the quoted recurrence, it would not have prevented other – perhaps more severe – failures affecting other machines.
Abubakar, Aisha; Bagheri Zadeh, Pooneh; Janicke, Helge; Howley, Richard (2016). "Root cause analysis (RCA) as a preliminary tool into the investigation of identity theft". Proc. 2016 International Conference On Cyber Security And Protection Of Digital Services (Cyber Security).
Babaoglu, O.; Jelasity, M.; Montresor, A.; Fetzer, C.; Leonardi, S.; van Moorsel, A.; van Steen, M., eds. (2005). Self-star Properties in Complex Information Systems; Conceptual and Practical Foundations. LNCS. Vol. 3460. Springer.
IATA (8 April 2016). "Root Cause Analysis for Civil Aviation Authorities and Air Navigation Service Providers". International Air Transport Association. Archived from the original on 8 April 2016. Retrieved 2017. Key steps to conducting an effective root cause analysis, which tools to use for root cause identification, and how to develop effective corrective actions plans.
Lewerentz, Claus; Lindner, Thomas, eds. (1995). Formal Development of Reactive Systems; Case Study Production Cell. LNCS. Vol. 891. Springer.
Manna, Zohar; Pnueli, Amir (1995). Temporal Verification of Reactive Systems: Safety. Springer. ISBN 978-0387944593.
Ohno, Taiichi (1988). Toyota Production System: Beyond Large-Scale Production. Portland, Oregon: Productivity Press. p. 17. ISBN 0-915299-14-3.
OSHA; EPA. "FactSheet: The Importance of Root Cause Analysis During Incident Investigation" . Occupational Safety and Health Administration. Retrieved 2019.
Sofema (17 November 2017). "Root Cause Analysis for Safety Management Practitioners & Business Area Owners". Sofema Aviation Services. Archived from the original on 17 November 2017. Retrieved 2017. Identify best practice techniques and behaviours to perform effective Root Cause Analysis (RCA)
Wilson, Paul F.; Dell, Larry D.; Anderson, Gaylord F. (1993). Root Cause Analysis: A Tool for Total Quality Management. Milwaukee, Wisconsin: ASQ Quality Press. ISBN 0-87389-163-5.
Research
Open access
Published: 08 November 2023
BMC Health Services Research 23, Article number: ()Cite this article
Abstract
Background
Root cause analysis (RCA) is a systematic approach, typically involving several stages, used in healthcare to identify the underlying causes of a medical error or sentinel event. This study focuses on how members of a Norwegian RCA team experience aspects of an RCA process and whether it complies with the Norwegian RCA method.
Method
Results
Conclusion
The findings of this study can help stakeholders better comprehend how an inter-professional RCA teamwork intervention can affect a healthcare organization and enhance the teamwork experience of healthcare staff while facilitating improvements in work processes and patient safety. Additionally, these results can guide stakeholders in creating, executing, utilizing, and educating others about RCA processes.
Peer Review reports
Introduction
Root cause analysis
The Norwegian regulatory regime for qualitative improvement and RCA
Fig. 1
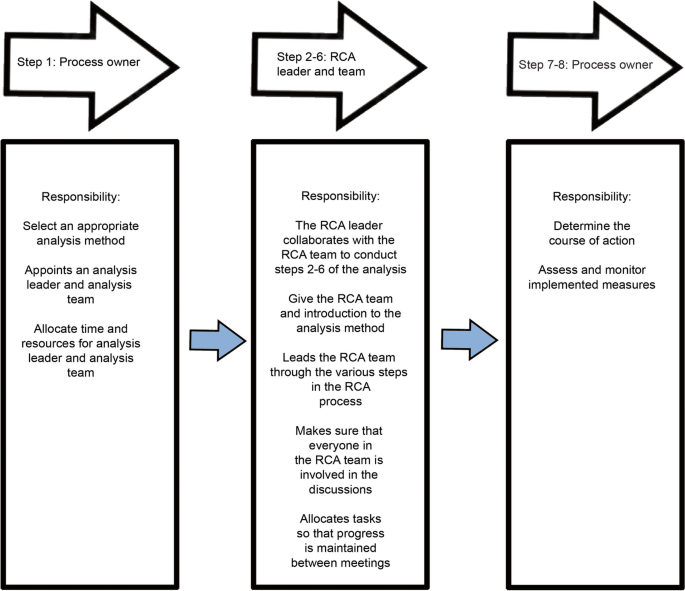
Roles and responsibilities in the Norwegian RCA process
Full size image
Methodology
Design
Interview data and relevant documents (Table 1) were collected and analyzed in separate phases of the research process. We identified patterns in the data material and extracted information and standard features to create an overall impression of the completed RCA process. Phase one explores the RCA team participants’ experiences with the pre-work before the RCA team meeting. In contrast, phase two explores the knowledge of the RCA members of the process, from the first team meeting to the completion of the final report.
Table 1 Overview of data and analysis methods used in the case study
Full size table
Setting and sample
Table 2 Characteristics of participants included in the interdisciplinary RCA team
Full size table
Data collection
The process of thematic coding
Table 3 Examples of the coding process in the interview dataset
Full size table
Ethical approval
Results
The results are presented first with a case description, illustrated by a timeline of the sentinel event and the subsequent RCA process (Fig. 2), and then with a description of three main themes and sub-themes we identified in the data. The first theme, referred to as “the management system,” outlines how the hospital management system manages sentinel events. The second theme, which we named “external and internal assessment,” focuses on how the RCA team perceived the role of “externals” and “internals” in evaluating the incident. Finally, the third theme, “being a team member,” describes how team members experienced carrying out an RCA process.
Fig. 2
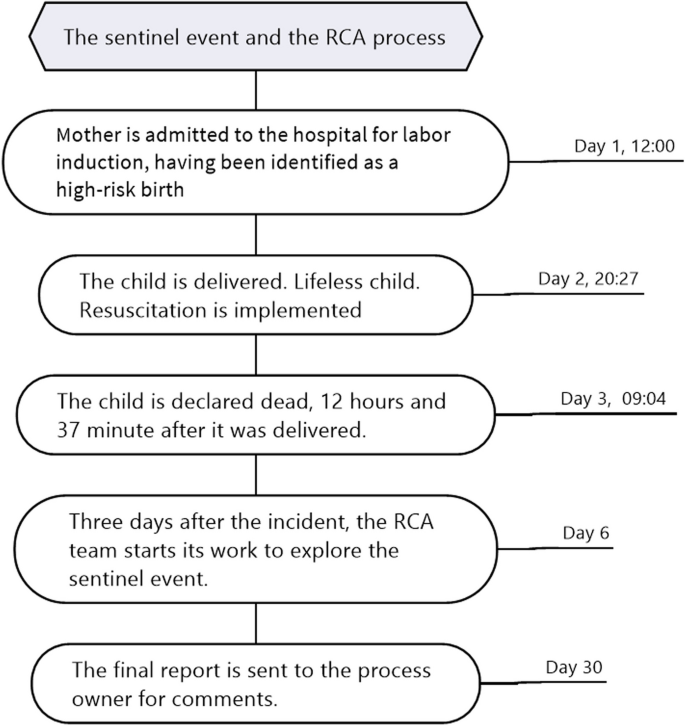
The course of the sentinel event and the subsequent RCA process
Full size image
Case description (The RCA team’s summary from the final report)
Theme: The management system
Quality management department’s role in the RCA process
The hospital trust, considered of medium size in Norway and overseeing four hospitals, had experienced several RCAs within a brief period concerning sentinel events during childbirth. Due to the gravity of the situation, the client manager was asked whether the quality department had the necessary resources and methodological expertise to conduct the RCA independently within the clinic. The Chief Quality Officer (CQO) acknowledged that they needed additional methodological expertise to carry out the RCA properly. The quality management department was brought in to provide expertise on the RCA method to ensure a methodical, correct, and professional approach. At the same time, employees working closely with patients were included in the RCA process. This was expected to facilitate knowledge-sharing and keep the process at a system level.
The quality management department played an active role in implementing national quality strategies and quality improvement requirements within the organization. However, there were different opinions within the organization on how the quality management department works with quality improvement. The quality management department had experienced resistance from some employees. Some employees were given feedback that they needed to better understand the quality management department’s role. In contrast, those who collaborated with them gained knowledge concerning their support function within the organization and quality improvement. The department appointed a contact person for each clinic to improve collaboration and communicate information about quality improvement tasks. However, some employees perceived the department as an ordering unit rather than a facilitator due to role confusion.
Scattered documentation
Theme: External and internal assessment
Composition of the RCA team
It emerged in the interviews that the RCA team was satisfied with the composition of the team. The RCA leader (QCO) decides the team composition in collaboration with the analysis team members and the organization managers. The RCA team comprised six members (as shown in Table 2); half of these were quality management department employees, while the other half consisted of medical experts from various departments. The team’s composition represented different aspects of the sentinel event. However, the team recognized that involving other professional groups, especially medical experts without close involvement in the incident, would have been beneficial. The “external- in-house” medical expert pointed out that other professionals, such as midwives, could have provided critical perspectives: “It might have been more appropriate to include other professional groups, such as midwives, to represent a more holistic composition of different professional groups.” The team members emphasized that working together during the process was seen as constructive, and they were able to come to a consensus.
The management department employees found the process challenging because team members had varying levels of experience with applying RCA. The same employees had participated in national training in the methodology and had conducted multiple analyses within the organization. All medical experts were familiar with the method through previous incidents in their clinics, but this was their first time carrying out a complete RCA process. The team members expressed that employees’ varying levels of experience with the RCA methodology could pose challenges in identifying root causes. Some team members suggested that increasing familiarity with the RCA method would be beneficial for fully understanding the RCA process within the organization. The team acknowledged that variations in experience with the RCA method could affect the quality of recommendations.
Police work interrupting the RCA process
Several members of the RCA team describe the police’s involvement in the case as disruptive to the internal RCA process. The police also had a very different approach from the RCA team and were perceived as brusque, foreign, and suspicious. “At first, they stepped in, and they were a little brusque, and they came in here and acted strange. They were rough, perhaps because they are used to communicating with people with something to hide!” Some employees felt that the incident was perceived as more serious when the police got involved. The police had turned up at the hospital for a crime scene investigation without reporting in advance. They expected this would be hidden from employees if evidence was tampered with. “Now we are standing outside—can you come and lock us in? Do not tell anyone we are here. In other words, so that they hide something before we come up.” The police then went in and seized evidence inside the crime scene.
One of the medical experts who had worked in other parts of the country gave feedback that it was common practice to report to the police in other healthcare organizations and noted that this element was handled entirely differently in this organization. The RCA team concluded that their organization had no culture and little knowledge and practice of reporting unnatural deaths to the police, which highlighted the need to work on implementation at both the clinic and organization levels.
Using colleagues to provide external medical expertise is seen as challenging for the process and the participants
In the RCA team’s mandate, it was requested by the process owner that a representative of the anesthetists should be part of the analysis team. The RCA team decided to extend this to include all specialist fields involved in the sentinel event. Previous RCA teams had brought medical expertise from outside the organization to offer an external perspective. The challenge in this RCA was that none of the other three hospitals in the organization had a neonatal ward and the expertise this provides. The RCA leader discussed with respective managers whether external medical expertise should be brought in. However, for this RCA, the decision was made to bring medical expertise from within the organization. They acknowledged that obtaining professional knowledge from within the hospital trust was not optimal, as other physicians could consider this decision in the organization as a mistake. At the same time, it was concluded by the RCA leader and the management that they could make use of medical experts who were not directly involved in the sentinel event. Therefore, they weighed the advantages and disadvantages and considered it prudent to use internal medical expertise in the RCA team. It was emphasized that the decision had been made because this was not an external inspection. They believed they had made the right decision by ensuring that the “external in-house” member had not been directly involved in the sentinel event.
RCA team members disagreed about using internal medical expertise, especially regarding colleagues considered “second victims” in the incident. The “external in-house” medical expertise pointed out that external medical specialists could provide a new perspective and make it easier to identify negative work patterns. Spending a long time in the same environment can lead one to become unaware of work habits. Team members suggested that the validity of this RCA could be improved by including external medical expertise and seeking expertise from outside their organization. Evaluating one’s colleagues in a relatively small environment was considered unconstructive in the implementation itself. The “external in-house” medical expert expressed that it would be emotionally challenging for the other members to evaluate the actions of their colleagues in the severe event. “I believe I was deeply emotionally detached when it came to those involved, their emotions, and everything related. My presence was primarily focused on the medical aspect of it.” The “external in-house” expert pointed out that internal medical experts should receive support and recognition for their work in the implementation. Still, a consequence could be that internal medical expertise could be affected by the emotional involvement of their colleagues.
The quality management department acknowledged that they had received feedback from their employees in the past that it was challenging to evaluate colleagues while also carrying out an RCA. “It is tough to evaluate colleagues in the way that we do. It is a heavy burden for those in the situations, also in the time afterward, because there are tough assessments and things that happen in ‘a blink of a moment’ that are analyzed thoroughly. It is demanding to be a colleague afterward. Because it hurts, it is a defeat. You have been involved in something challenging, and then it must be assessed afterward, and it is easier if you do not have a relationship afterward.” They pointed out that assessing a situation was easier when there was no prior relationship with those involved.
Theme: Being an RCA team member
Role challenges
Ambivalence about being an RCA team member
The roles and motivations of the RCA team members were diverse and complex, with some expressing ambivalence about their participation. On the one hand, they felt a sense of obligation towards the families who had experienced a loss and their colleagues who were also impacted. “I think we owe it to those who have experienced losing their child, as well as health personnel who have experienced this.” They valued the educational aspect of the process and appreciated the chance to work with other experts and learn from resource personnel within the organization. They believed that carefully examining sentinel events, particularly those with significant consequences, was critical. Nonetheless, they found it challenging to scrutinize their colleagues, especially when they discovered mistakes. Some members initially hesitated to participate but felt compelled because the professional pool was too small to make it practical to choose other team members. Some medical experts agreed to join the RCA because they were confident that they would not uncover errors made by their colleagues.
Discussion
The results indicate that the RCA team faced various challenges during the RCA process, including the difficulty of being neutral, role challenges, ambivalence about being an RCA team member, and the additional burden on time and resources. Although the analysis process was demanding, all members expressed engagement in participating in the RCA team. Further, the study findings indicate that there can be significant challenges in applying the Norwegian RCA guidelines as laid out by health authorities. This case shows that the management system presupposes clear descriptions of responsibilities, and easily accessible information, which can be challenging to achieve in this complex environment. At the same time, we found that challenges related to medical documentation (scattered documentation), the role of the police, and the ideal of neutrality in the assessment of colleagues (external and internal assessment) indicate the need to problematize certain recommendations in the Norwegian RCA guidelines.
Members of the RCA team expressed that evaluating the case and their colleagues was emotionally challenging. Therefore, being neutral and having no other interest besides increasing patient safety was difficult. This reality deviates from the idealistic approach in the Norwegian RCA guidelines, which requires the RCA process to be carried out with neutrality on the part of the participants. Colleagues of the RCA team had experienced both being the second victim in the case and being inflicted with a new trauma when the RCA process was initiated. Police investigations and media exposure also made it challenging to carry out the RCA in the organization. We argue that expecting neutrality in an RCA process is unrealistic because the issues being investigated involve people with emotions. In some cases, people involved may have a vested interest in the outcome of the analysis. Additionally, the emotional impact of the incident may make it difficult for individuals to remain detached and impartial. All these factors can make maintaining neutrality throughout the RCA process demanding, with a risk of inaccurate analysis.
Our results also revealed internal disagreement concerning which deaths should be reported to the police. The organization had no established routines for reporting cases like this to the police. The involvement of the police leads to fear of external supervision. Employees and members of the RCA team experienced that the police investigation disrupted the RCA process and alienated them. Part of the explanation could be that this was experienced as a new way of handling death. At the same time, it was pointed out by the RCA team that one had to be able to see the police involvement from the viewpoint of the parents who had unexpectedly lost their child and who wanted answers as to why their child had died. This consideration was challenging to acknowledge for the employees and some RCA members when the police started their external assessment of the event.
Implications for practice
Study strengths and limitations
Future research and development
Future development could include a national register for RCA documentation to track trends and promote learning. The lack of official documentation of the RCA process and final report means that only a few people have insight into the process. Making the final report official and anonymous could increase transparency and trust within hospitals and reassure patients and their families. Interviews are critical for understanding an incident’s cause, but recall bias often delays or affects them. Gathering information from all relevant parties while the incident is still fresh is crucial for successful documentation. The involvement of police in the RCA process can delay interviews and create a more serious atmosphere, which can affect the process. To improve the RCA process, individual professionals should increase awareness and efforts to achieve documentation by providing adequate resources, clear mission statements, and coherent policies. Involving permanent members from the quality and safety department staff in several RCA processes can provide a better basis for comparison. Finally, the Norwegian Board of Health Supervision emphasizes collecting information from all relevant parties, including patients and their families.
Conclusion
This study is one of few studies that have explored RCA team experiences during an RCA process and whether there is adherence to the Norwegian RCA method. The results may inspire healthcare organizations, health authorities, quality and patient officers, and RCA teams to improve the RCA guidelines further and learn from this case. This study has shed light on three critical RCA team experiences: Firstly, the intricacies of the healthcare management system, particularly the role played by the quality management department, underscore the need for seamless integration of RCA into everyday practices. The integration is vital for enhanced support and guidance to employees during crises.
Secondly, the delicate balance between internal and external assessments in the RCA process highlights the value of embracing diverse perspectives and expertise. This inclusivity is essential to obtain a comprehensive understanding of sentinel events.
Lastly, the challenges and ambivalence encountered by RCA team members as they evaluate their colleagues and navigate their roles emphasize the need for clearer communication and robust support mechanisms.
These experiences have practical implications for healthcare organizations, RCA team, and professionals. It is, therefore, necessary to streamline the management system, promote a culture of continuous learning and support, and ensure that RCAs benefit from both internal and external insights. To address these issues, we recommend a renewed focus on education and training, improved collaboration between internal and external stakeholders, and more robust support system for RCA team members.
In the broader context of patient safety discourse, these experiences emphasize the need for a proactive and holistic approach to quality improvement. By addressing these key experiences, healthcare organizations can move closer to a safety culture where patient well-being remains paramount. Ultimately, being aware of and acting upon these critical RCA team experiences can hopefully lead to safer and more effective healthcare practices for all.
Availability of data and materials
The data generated and analyzed in the current study are not publicly available due to Norwegian privacy legislation and the form signed by the participants about the study`s privacy. The data generated are available from the corresponding author on reasonable request.
References
Acknowledgements
We give thanks to the health professionals participating in this study.
Funding
Open access funding provided by Norwegian University of Science and Technology The Norwegian University of Science and Technology funded the study. The funding institution did not make decisions regarding study design, data collection, analysis, interpretation, or writing of the manuscript.
Author information
Authors and Affiliations
- Department of Health Sciences, Ålesund, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology, Larsgårdsvegen 2, Ålesund, 6025, Norway
Silje Liepelt & Ralf Kirchhoff
Faculty of Health Sciences and Social Care, Molde University College, PO. Box 2110, Molde, 6402, Norway
You can also search for this author in
You can also search for this author in
You can also search for this author in
Contributions
All authors designed the study. S.L. collected the data and analysed the data in collaboration with H.S. and R.K. All the authors contributed to the manuscript revision. All authors read and approved the final manuscript.
Corresponding author
Correspondence toSilje Liepelt.
Ethics declarations
Ethics approval and consent to participate
According to the Declaration of Helsinki, the study participants ‘rights, dignity, and privacy were ensured. The participants received oral and written information about the study. Written informed consent was obtained from all the participants. Participation was voluntary, and the participants could withdraw without explanation. The Regional Committee for Medical and Health Research Ethics (REK) concluded that the study (ref. #195549), categorized as a quality improvement project, did not require REK approval as it falls outside the scope of medical and health research under the Health Research Act. The handling of personal information in the project (project number 562024) was conferred with NSD according to requirements in the act relation to personal information and GDPR.
Consent for publication
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Rights and permissions
Reprints and permissions
About this article
Cite this article
Liepelt, S., Sundal, H. & Kirchhoff, R. Team experiences of the root cause analysis process after a sentinel event: a qualitative case study.BMC Health Serv Res 23, 1224 (2023). https://doi.org/10.1186/s12913-023-10178-3
Received21 June 2023
Accepted18 October 2023
Keywords
RCA is the abbreviation for Root Cause Analysis. In the dynamic landscape of modern industries, where efficiency, safety, and quality are paramount, the ability to identify and address the root causes of problems is a skill that cannot be overstated. Root Cause Analysis (RCA) is the systematic approach that holds the key to understanding the origins of issues, incidents, and failures in various fields, from healthcare and manufacturing to aviation and information technology. This blog post serves as a comprehensive guide to RCA, delving deep into its definition, the pivotal role it plays in preventing the recurrence of problems, and an outline of what you can expect to explore as we journey through this exploration.
Root Cause Analysis is not just a problem-solving technique; it is a mindset, a culture, and a discipline that empowers organizations to dig beneath the surface of apparent issues and unveil the underlying factors that drive them. By doing so, RCA not only resolves immediate challenges but also provides the insights needed to fortify processes, enhance safety, improve product quality, and ultimately elevate the performance of individuals and organizations.
Throughout this post, we will navigate through the intricacies of RCA, dissecting its various methods and tools. We will explore real-world examples of how RCA has been instrumental in averting disasters, optimizing operations, and saving lives. Moreover, we will discuss the diverse industries in which RCA has found its invaluable application, shedding light on its adaptability and universal significance.